Breast Augmentation- Patient 176
Learn about patientBreast Augmentation- Patient 176

Breast Augmentation- Patient 175
Learn about patientBreast Augmentation- Patient 175
Breast Augmentation Revision – Patient 107
Learn about patientBreast Augmentation Revision – Patient 107

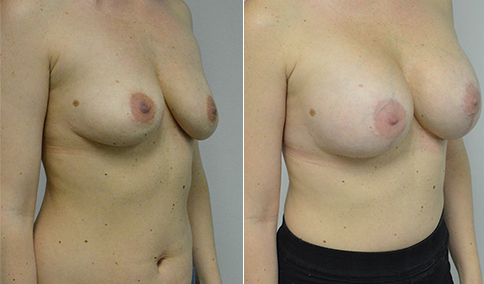
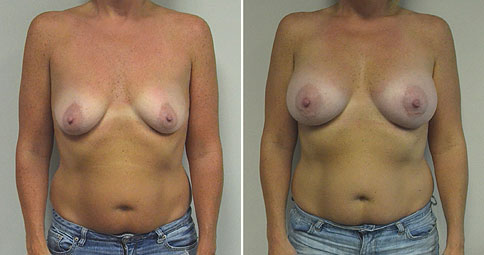
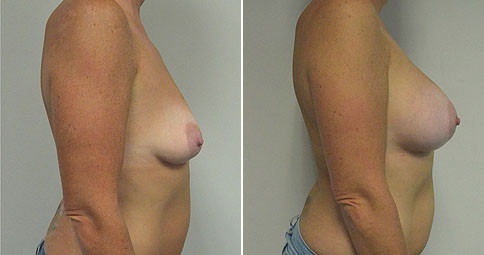
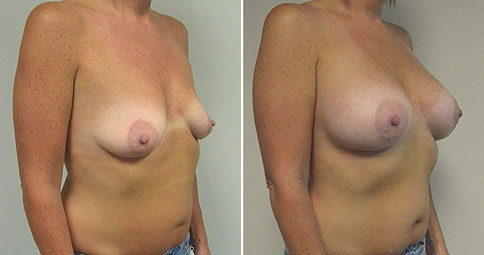
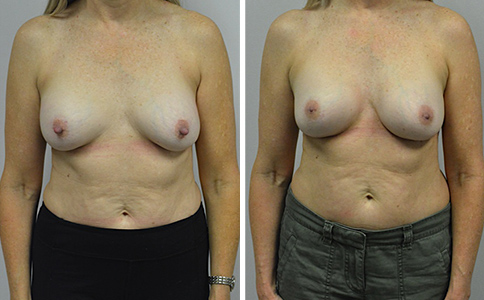
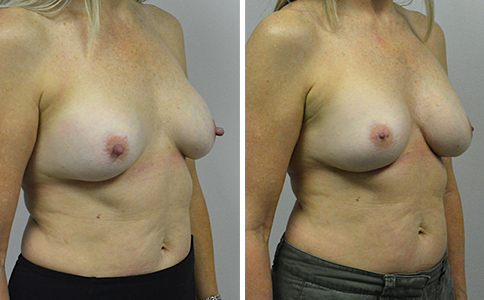
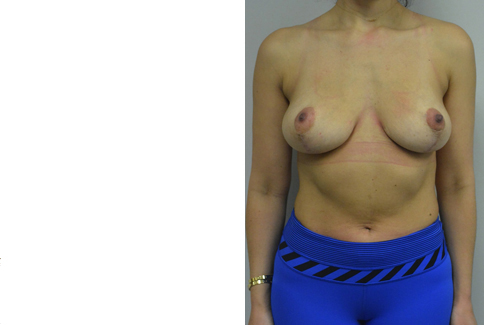
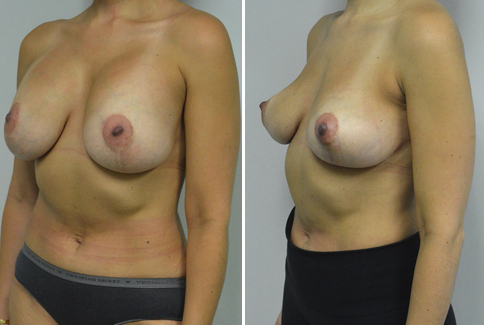
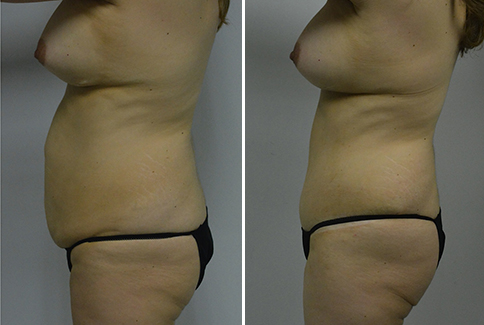
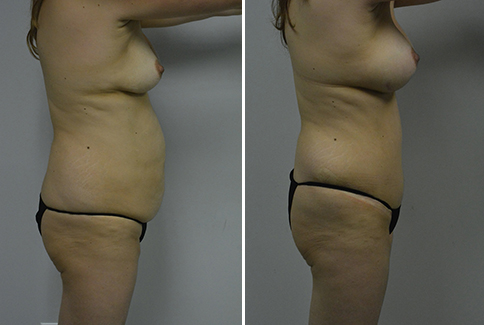
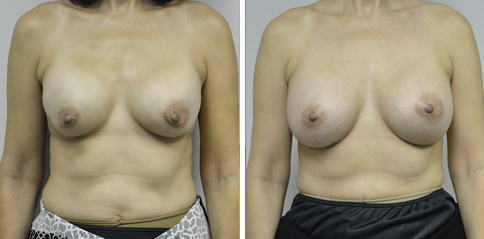
A challenging case of a woman in her early 30’s with a right implant deflation, and bilateral fold malposition. She had breast augmentation down south when she was 21. She was small C at the time and wished to be a full C. Her records were obtained and show that 500 cc high profile saline implants were placed below the muscle through a periareolar incision. She was a 34D-DD after her surgery and was having issues with back and shoulder pain due to the new size of her breasts. She came in to see us after her right implant had deflated. She did not like her breasts falling off to the side and the loss of fullness in her upper breast. She wished to be smaller but still a full C. Our plan was to deflate her left saline implant in the office and let her breast recover for at least 4 weeks before surgery. In the mean time she made the happy discover that she was again pregnant so we went ahead and deflated her saline implant in the office so that her breast would not stretch even more with her pregnancy and then waited until 6 months after her pregnancy to let her breast resume its normal volume and perform her surgery. We sized her again in the office and she liked a 375-400 cc volume the best. She is 5’7” and 145 lbs. Typically the volume of an implant will drop into the lower breast after it has been stretched with pregnancy or prior implants and not give lasting fullness in the upper breast. In order to help maintain some fullness in her upper breast, she elected for a round, high profile silicone gel implant. Texture was chosen to help stabilize the implants and decrease stretching of the lower breast and lateral shift. The Sientra gel is “form stable” in their round implants and is the most cohesive of the choices so this was selected for her. A 415 high profile textured round implant was placed after performing a capsulorrhaphy ( a suturing internally to tighten the prior implant space which had been overly stretched) and a bilateral mastopexy. We had Seri Scaffold available in the OR to reinforce the internal capsulorraphy repair but is was not needed.
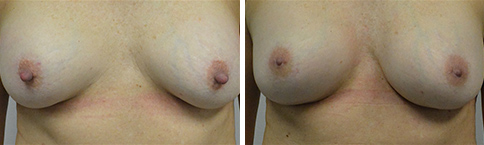
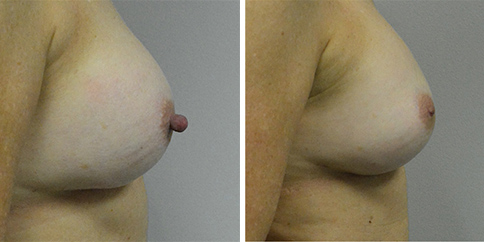
Our patient is now seen 7 months after her surgery. Her scars continue to fade and the shape has “settled”. The lateral capsulorraphy (repair of the lateral pocket) and textured form stable implant has prevented lateral shift ( the implants dropping to the side) which is demonstrated in a photo with her lying down flat. Her breasts remain soft, and she continues to like the “feel” of the silicone gel implants better than the saline implants. She continues with the topical silicone application- her scars are doing well for 7 months, but will typically continue to fade and improve over the next 18 months.
Breast Augmentation Revision – Patient 106
Learn about patientBreast Augmentation Revision – Patient 106

A fitness instructor in her early 50’s who came in to evaluate her implants and also to address problems with her nipples. She initially had surgery 26 years earlier and reports significant bruising afterwards, followed by a fairly rapid development of hardness around her implants. The hardness of the implants (capsular contracture) made it uncomfortable to lie on her stomach. She was also bothered by “long nipples” that were overly prominent in her clothing. She wears silicone nipple shields to hide them. They are also very sensitive in the shower and against her clothing. Given the length of time since her original surgery I obtained an MRI which showed that both implants were ruptured.
Decisions to make: Replace or remove? She likes filling her bra without the padding and wants to replace the implants. Saline or silicone? Her tissues are thin, and she does not want the additional wrinkles and ripples which may be more noticeable with saline implants.Keep the implant above the muscle or place it below the muscle? She does not want to see motion of the implants when she tightens her pectoralis muscles (animation) and would prefer to keep the implants above the muscle. Our usual decision would be to place the implants in contact with fresh tissue in a new plane below the muscle but I felt that I might be able to make a new space between the implant capsule and the muscle ( a “neosubcapsular” space) so the implants would be in contact with fresh tissue but still above the muscle. Texture or smooth surface? Texture can decrease dropping and lateral shifting of the implant with time but can increase the risk of late seroma and pseudocapsule formation. Because she is so physically active, she would theoretically be more at risk for seroma and pseudocapsule with the texture so she elected for the tradeoffs of the smooth.
Size? She is 5 1 ½ and 118 lbs. Her operative report was obtained and listed a 175 cc implant on her left and an adjustable implant on her right but did not mention its size. After discussion of the options she elected for 250 cc implant on her left, which we sized her in the office by adding 75cc sizing shell to her existing breast so she could see how this looked in a bra. Our plan was to have a range of sizes available for the right side and to decide in the operating room.
Choice of nipple reduction procedure: The “standard” approach that is taught is to amputate the top of the nipple and let this heal in. Although this does reduce the height of the nipple papule it cannot reduce it’s diameter. We elected for a top hat flap procedure, which does not leave any raw areas to heal in and also reduces the diameter and height of the nipple papule. Remove and replace the implants immediately or leave them out for 3 months before replacing? Capsular contracture can be difficult to treat, and can havea high recurrence rate with immediate replacement of the implants- as high as 70% in some studies. The causes of capsular contracture are still being debated. A common cause may be biofilm, where bacteria gets on the implant and “walls itself off” (like tartar on your teeth that the dentist scrapes off) so that the body can’t fight it. In a situation like this, simply replacing the implant does not give the body a chance to clear the bacteria and the risk of it spreading to the new implant and causing a contracture is high. I have had the best success in these cases by leaving the implant out for 3 months prior to replacing it. But a hematoma (collection of excessive blood around the implant) can also stimulate a capsular contracture and given her history of significant bruising after her original surgery this seemed more likely in her case. I am not as worried then about immediate replacement of the implant and this is what she elected.
Surgery: Her old scars were two fingerbreadths above her existing inframammary fold and were felt to be too high and had not healed satisfactorily. I felt it best to place new incisions in the proper location along her existing inframammary fold and this was discussed and approved by her. I was fortunately able to develop a neosubcapsular pocket, below the old breast capsule but above the muscle. In this way the implants could be kept in the subglandular position as per the patients request, but in a new “space” in a fresh plane of tissue. The ruptured implants were removed. The 250 cc round smooth moderate profile plus silicone gel implant was placed on her left, and was best matched with a 275 cc round smooth moderate profile silicone gel implant on her right. She is now seen nearly 3 months after surgery. Although it is early, her breasts have remained soft and she can now lie comfortably on her stomach. She has not lost nipple sensation, but no longer has the hypersensitivity in the shower and from her clothing.

Breast Augmentation Revision – Patient 105
Learn about patientBreast Augmentation Revision – Patient 105

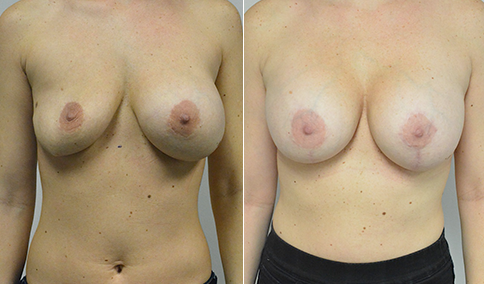
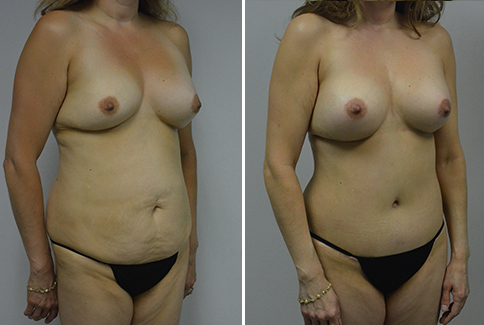
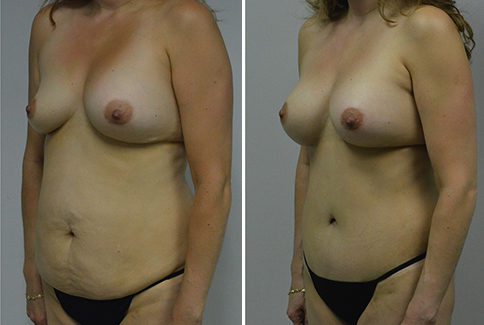
A mother of 3 in her mid 40’w who was 21 years after saline breast augmentation when she developed a sudden deflation of her right breast implant. She did not have her records,so we had to make an educated guess and have a range of implants available in the operating room. Her left implant was weighed upon removal and was determined to be filled to 392cc. She did not have a history of capsular contracture (firmness of the breast due to tightening of the scar tissue around the implant, often felt to be from “biofilm”) so I felt comfortable with immediately replacing her implants. She elected for silicone gel implants, and was replaced with 375 cc cohesive round silicone gel high profile implants, which are similar in dimensions to her current implants. She is shown before and again, 8 months after surgery. She is especially pleased with the more natural feel of the implants, compared to her prior saline implants. I was able to use her original infra mammary incision. She had an abdominoplasty at the same time. Of course the breasts are “sisters and not twins” with her right nipple being higher than her left before and after surgery.

Breast Augmentation Revision – Patient 104
Learn about patientBreast Augmentation Revision – Patient 104
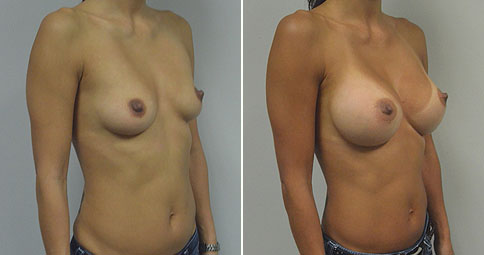

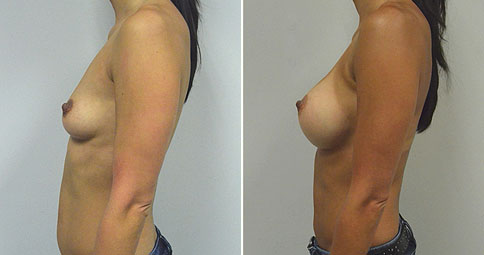
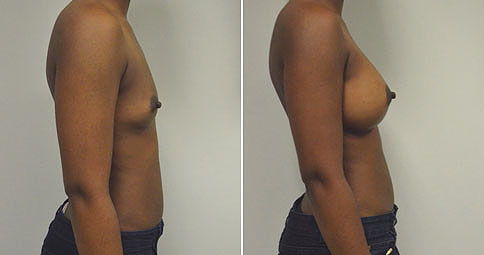
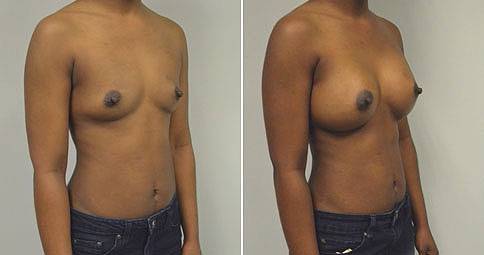
An Asian professional in her early 40’s. Mother of one. Now shown 14 months after bilateral partial sub pectoral breast augmentation with 375 cc round smooth silicone gel moderate profile plus implants placed through an inframammary (breast fold) incision in a partial sub pectoral (below the muscle) location. She is 5’4″ and 118 lbs.
An Asian professional in her early 40’s. Mother of one. Initially shown 14 months after bilateral partial sub pectoral breast augmentation with 375 cc round smooth silicone gel moderate profile plus implants placed through an inframammary (breast fold) incision in a partial sub pectoral (below the muscle) location. She is 5’4″ and 118 lbs. It is said that 90+% of women after breast augmentation wish that they had “gone larger” but that is not always the case. Some women wish to downsize. This woman initially selected the 375 cc implant after discussions and sizing in the office. She was ok with the look in clothing, but always felt a little self-concious in a bathing suit. Then her liftestyle changed and she began to spend more time at the gym. The tight gym clothes accentuated her breasts to the point that she felt that they were too full. She decided after 2 1/2 years to return to the operating room and down-size to a 275 cc moderate profile plus round smooth silicone gel implant. Her original incision at the breast fold was used, and I tightened her lower pocket by performing an excision of the breast capsule in the lower portion and anchoring it to the periosteum (covering) of her rib (this is called a capsulorrhaphy). The “pocket” that the implant was in would be too large for the new implant otherwise. She is now seen 7 1/2 months since this second procedure. Her breasts are fuller than before her initial surgery but now seem absolutely natural to her in her workout clothes and in a bathing suit. It is a cautionary tale, that even with careful discussion of the tradeoffs and sizing in the office, not everyone “wishes that they had gone larger”
Breast Augmentation Revision – Patient 103
Learn about patientBreast Augmentation Revision – Patient 103



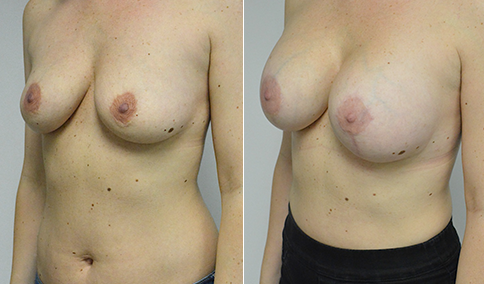
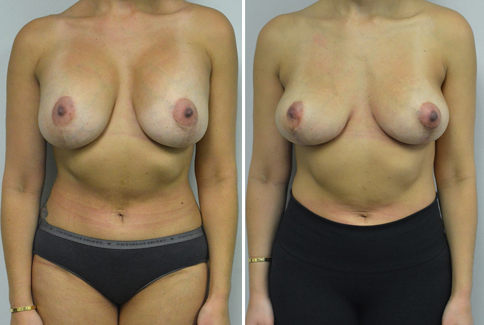
A woman in her mid 30’s who describes herself as a 32 DDD. She had breast implants and a breast lift in Texas in 2011 with 375 cc silicone implants. She feels that she is too large, and does not like the superior fullness in her upper breasts from the implants. Her nipples are properly positioned at 21 1/2 cm from the sternal notch, but she has an increased distance from the nipple to the breast fold. There is always a worry about the blood supply to the nipple when a patient has had previous surgery in this area, so not having to move the nipples is a relief. She had an inverted T mastopexy using her previous scars,, along with removal of her implants. She is shown again, 2 months after surgery. She had enough breast volume remaining to be pleased with her “C”cup breast after surgery. Her scars have also been improved slightly, and will continue to fade over the next 2 years. The imprints on her skin are from the silicone pads that we are having her wear after the surgery to improve her scars.
Our patient is seen again, now 5 months after surgery. Her scars continue to fade with the silicone pads, and the breasts are “settling in” to their new shape.

Breast Augmentation Revision – Patient 102
Learn about patientBreast Augmentation Revision – Patient 102


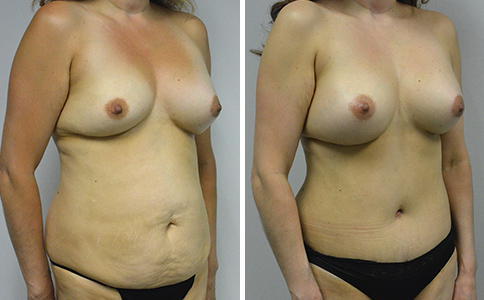
A mother of 3 in her mid 40’s who developed a sudden implant deflation on her right side, 21 years after having saline implants. She did not have her original records. Her left intact implant was weighed at the time of removal, 392 gms. They were both replaced with 375 cc smooth round high profile cohesive silicone gel implants. She had an extended abdominoplasty along with repair of an umbilical hernia. Seri Surgical scaffold was used to reinforce the umbilical hernia repair at the time of surgery. EXPAREL was used at the end of surgery to decrease postoperative pain. She is shown before and again, 4 months after surgery. There is typically still some swelling in the lower abdomen for the first 6 months, so she may decrease a little more in the lower abdomen. She reports that she is down from a 10 to a 6 dress size. The oblique view demonstrates the periumibilical hollow and champagne groove sculpted in the fat at the time of surgery.
Breast Augmentation Revision – Patient 101
Learn about patientBreast Augmentation Revision – Patient 101

A mother of 2 in her early 50’s who had bilateral implant rupture diagnosed on MRI. She is 5’5″ and 136 lbs. She initially had surgery in Boston 19 years before, but was unable to obtain her records. She remembers significant bruising after her original surgery and rapid development of firmness of her right breast, which softened a little over the following years. On examination, she was shown to have capsular contracture on both sides. Her incisions were initially placed through an incision around the areolar. Treating a capsular contracture can be challenging. Many capsular contractures may be the result of Biofilm (bacteria that attaches to the implant and walls itself off so the body cannot fight it properly) and may best be treated by leaving the implants out for a few months while the body clears the bacteria, before replacing the implants. Some recent longitudinal (long term) studies have suggested a higher risk of capsular contracture when the implant is placed through an incision around the nipple or in the axilla. Another option may be to use Acellular dermal matrices such as Strattice but these involve using an animal product and additional expense. Her history of severe bruising followed by a contracture which softened a little with time seems more consistent with a hematoma as the cause. She elected for bilateral implant removal with creation of NeoSubpectoral pockets bilaterally and placement of 350 cc round textured cohesive silicone gel implants through an infra mammary (at the breast fold) incision. A “neosubpectoral” pocket involves carefully making a new space between the capsule around the implant and the pectorals muscle. Her implants were “riding high” and the new pocket was made slightly lower. She is shown just before and again, 6 weeks after surgery. Her breasts remain soft. She is not “out of the woods yet” in terms of the risk of developing another contracture, but we are hopeful that we have solved her problem.
At 4 1/2 months after surgery the breasts remain soft and without recurrence of her capsular contracture.




Cosmetic & Plastic Surgery Specialist
"I treat my patients like I would treat
- Jonathan D. Hall, MD, FACSmembers of my own family."
Schedule Consultation