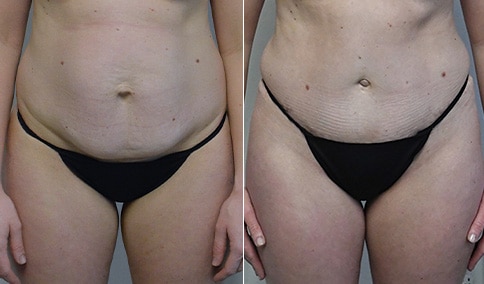
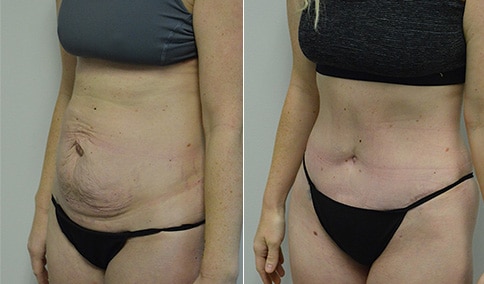
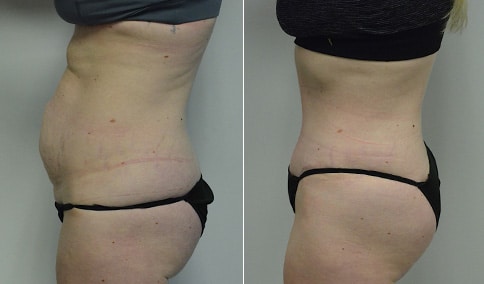
A mother of 2 in her mid 50’s who is bothered by rolls of skin in her abdomen which are difficult to hide in fitted clothing. She is 5’4 ½ and 147 lbs and is shown before and again, 4 months after an extended abdominoplasty. Her scar is low, in a thong position, and a periumbilical hollow and “champagne groove” above the umbilicus were sculpted at the time of her surgery. Exparel was used to decrease her need for narcotics after surgery.
Although swelling will continue to improve for 6 months after abdominoplasty she is already thrilled with her improvement.
Update: Our patient is seen again 16 months after her surgery. The sculpting of the abdominal flaps is seen with a beautiful “champagne groove” and hollow around the umbilicus giving the abdomen and even more beautiful appearance after surgery.
















































Cosmetic & Plastic Surgery Specialist
"I treat my patients like I would treat
- Jonathan D. Hall, MD, FACSmembers of my own family."
Schedule Consultation