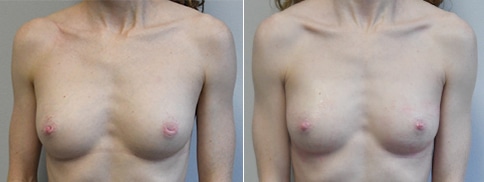
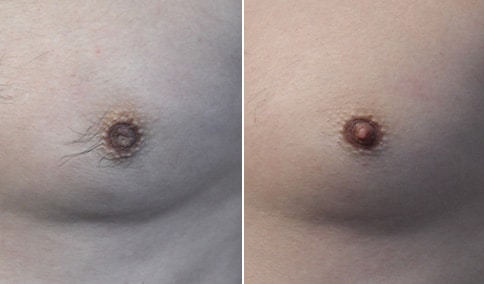
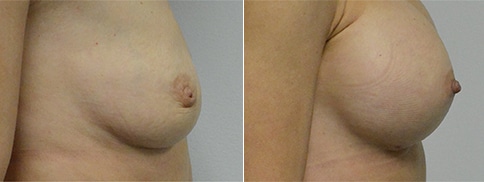
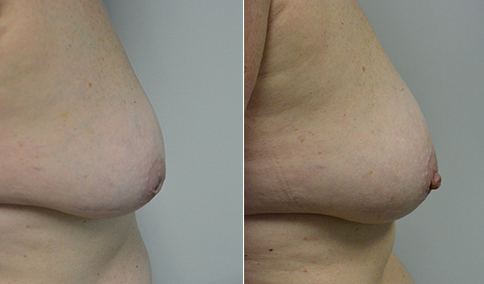
A mother of one in her later 20’s who is bothered by inverted (retracted) nipples. Her right side was moderate and her left side severe according to the classification of Han and Hong. According to Han and Hong, mild or grade I retraction is where the nipple can be pulled out easily and maintains its projection without traction. Moderate or grade II is when the nipple can also be pulled out manually, although not as easily as with grade I and has difficulty maintaining its position with a tendency to retract. Severe inversion, or grade III the nipple is difficult to pull out manually. Nipple retraction is caused by short and retracted milk ducts. To correct this, these ducts are divided under local anesthesia with a special blade through a micro incision and held out to length temporarily with a traction suture while healing is taking place.
She had initial correction with the micro-incision technique under local anesthesia in the office. Although it is rare, she did not achieve satisfactory correction with the first procedure and continued to have some retraction. We returned when she was available for surgery 10 months later and she had a second micro-incision technique on each side. She is shown now at 6 weeks after this second procedure, and has maintained a normal nipple projection. She is happy to “feel normal” again and “confident” about the appearance of her breasts after correcton.































Cosmetic & Plastic Surgery Specialist
"I treat my patients like I would treat
- Jonathan D. Hall, MD, FACSmembers of my own family."
Schedule Consultation