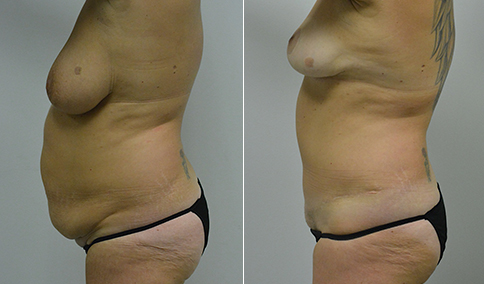
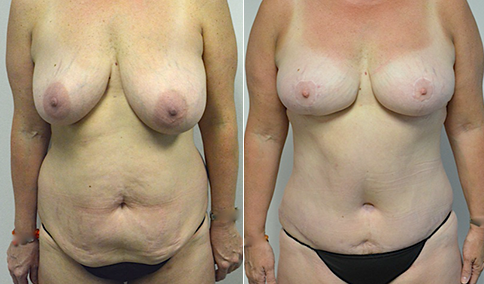
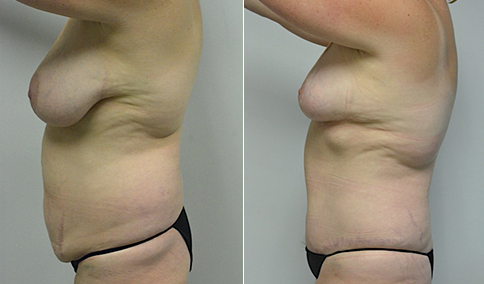
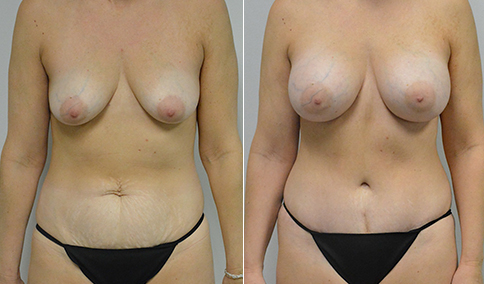
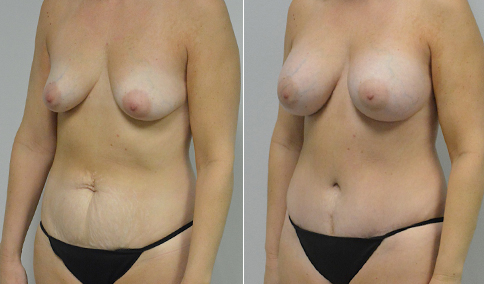
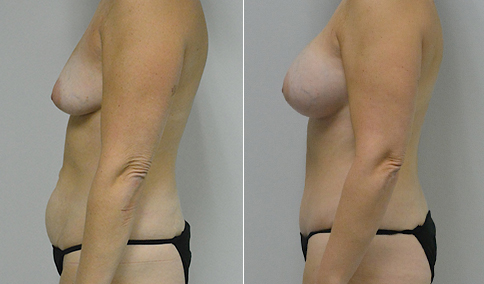
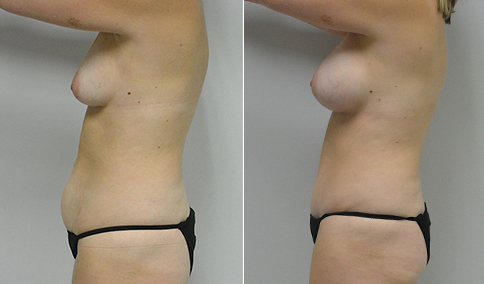
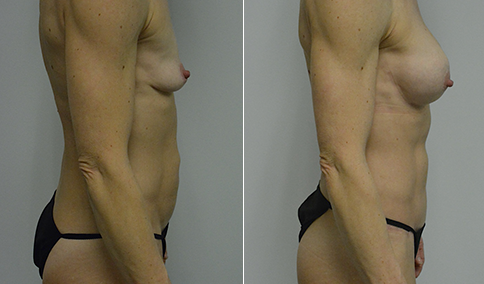
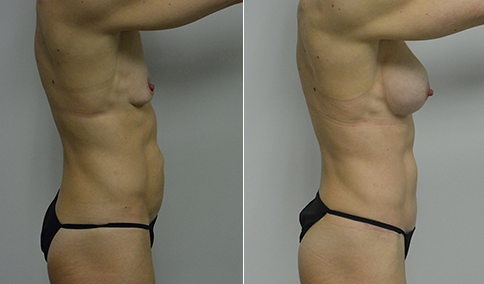
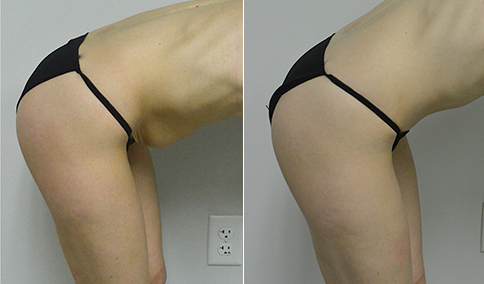
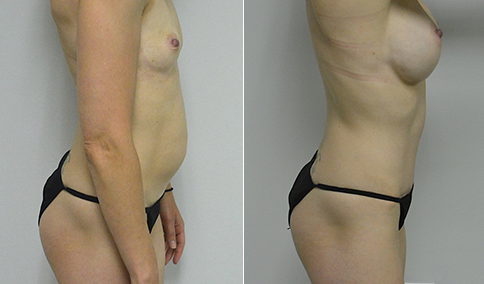
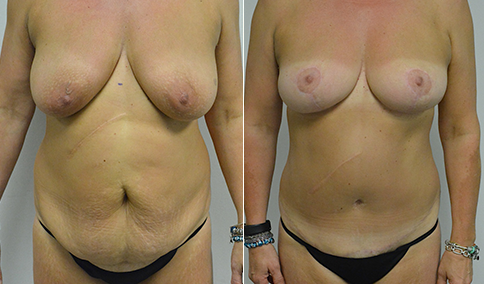
A body builder and mother of 1 in her late 40’s who is bothered by a deflated appearance of her breasts, as well as wrinkling and looseness of the abdominal skin above the umbilicus. She gained and lost 70 lbs with her pregnancy, and recently lost another 30 lbs. She is 5’2” and 122 lbs. She is shown before and again, one year after bilateral dual plane breast augmentation with 300 cc round textured high profile silicone gel implants placed through an inframammary incision, combined with an abdominoplasty.
The decisions for her case are complex and deserving of discussion. Body builders are a unique population because they have very thin tissues. The implant can be places above the muscle so that no motion is seen as the pectoralis muscles are triggered, but the breasts do not age as well, and because her tissues are so thin might show rippling in the cleavage area. A “dual plane” placement allows the implant to be below the muscle in the upper breast where it has more padding and coverage, but above the muscle in the lower breast to that the implant can settle more with the breast an avoid a “waterfall” effect with the breast dropping off of the implant mound. In patients who have had significant weight loss, the breasts will tend to drop to the side more because of decreased elasticity. This can be even more of a problem with body builders who are constantly triggering the pectoral muscle. So texture of the implant can decrease the risk of this potential lateral shift and stretch. The three implant companies have different degrees of “aggressiveness” of the texture, and late seroma formation, and pseudocapsule formation may be more likely with the more aggressive textures. So we chose the company with the texture that is the least aggressive ( but has been shown to have the same “grip” known as the coefficient of friction). At one year her breasts remain stable and have not shifted to the side.
In her abdomen, she could consider a “reverse abdominoplasty” which would place a scar under the breasts and at the upper abdomen but has not been as successful in my hands in tightening the skin. “Floating” of the umbilicus would avoid a scar around the umbilicus and a vertical scar in the lower abdomen but would not tighten the upper abdomen, which is her problem area. After much discussion and viewing of photographs of other patients, she elected for a traditional abdominoplasty with a small vertical slit closure scar in the lower abdomen as being a worthy tradeoff for tightening of the overall abdomen. These scars will typically continue to fade and improve over the next year. She is thrilled with her result, and busy preparing for her next competition.
















Cosmetic & Plastic Surgery Specialist
"I treat my patients like I would treat
- Jonathan D. Hall, MD, FACSmembers of my own family."
Schedule Consultation