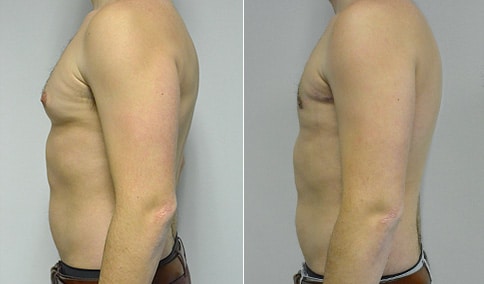
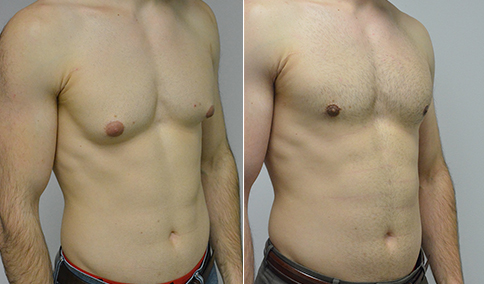
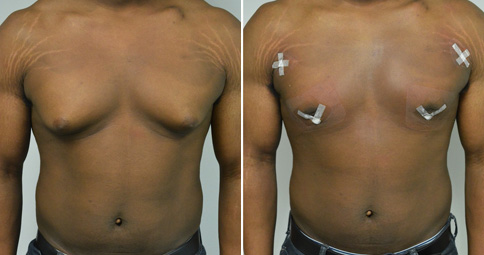
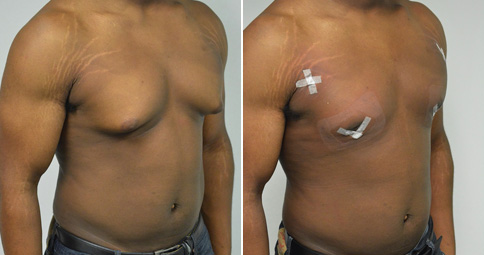
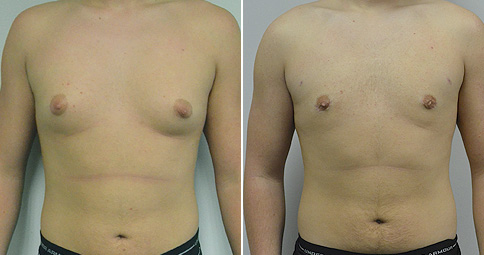
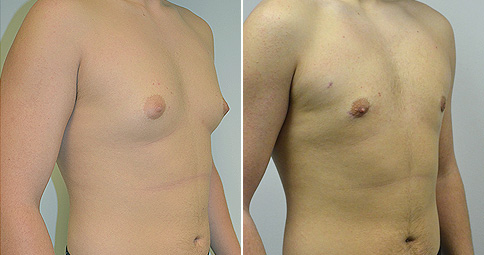
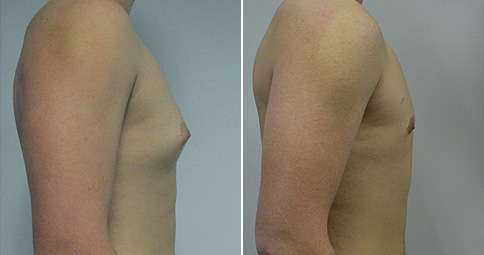
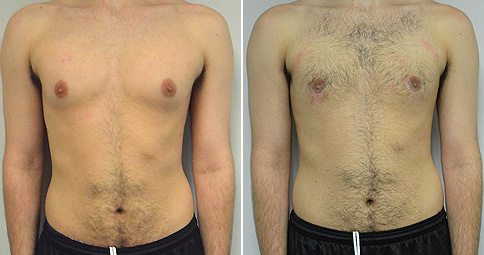
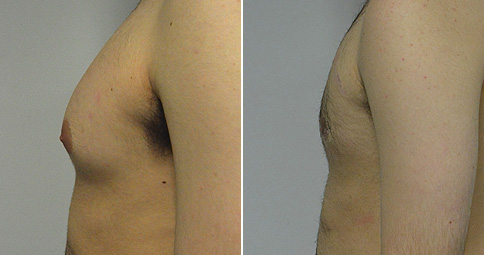
An early ( 6 week) follow-up on a man in his early 30’s who first noted gynecomastia in his mid 20’s. He has had negative endocrinology testing and a negative testicular exam (testicular tumors can be one cause of gynecomastia). He is bothered by the appearance of his chest with his shirt off but also in fitted shirts and golf shirts. He wears extra shirts to camouflage his chest. He did take over the counter supplements for weight lifting, and that may have been the cause. He is 5’ 11” and 166 lbs and is shown just before and again, 6 weeks after Power Assisted liposuction of his chest using the S.A.F.E. technique ( S uction A spiration F at E qualization). After liposuction fluid is placed in the chest, then external ultrasound is applied to soften the fat. Then a cannula with fins is used first without suction to mechanically disrupt the fat. Then liposuction with a normal liposuction cannula is used. Any residual breast tissue that remains is excised through an incision around the areola- in his case about ½ ounce of tissue was excised from each side. Then the finned cannula is used again to smooth and equalize the remaining fat. Scars are at their thickest and reddest at the 6-week mark and he has been wearing paper tape to protect his incisions. We can see a little redness of the skin from the tape and from the scars, which will now fade over the next 6-12 months. The hands on head view shows the excellent contour that has been obtained and brings the gynecomastia into view before and shows the complete resolution after his surgery. He told me that he is so happy and relieved to have a normal appearing chest again. A tattoo on his arm has been blurred for his privacy. The photos are otherwise not retouched.
Update: Our patient is now seen 8 months after surgery. His contour remains excellent and his scars have continued to fade. He tells me that his only wish is that he had done this sooner. He is thrilled to be able to take his shirt off at the beach and look normal. And he is no longer bothered by the appearance of his chest in fitted shirts.


































Cosmetic & Plastic Surgery Specialist
"I treat my patients like I would treat
- Jonathan D. Hall, MD, FACSmembers of my own family."
Schedule Consultation